



Dear Readers,
I hope you had a restful weekend - especially if you weren’t working. If you were, thank you, and we hope it wasn’t too busy. A few publications from the last few weeks caught my eye, and I’ll share them with you here.
All the best,
Danny
Neonatal Herpes Simplex Virus

A baby girl was noted to have vesicular skin lesions immediately after spontaneous vaginal delivery at 32 weeks gestation. Her 37-year-old mother had a premature rupture of membranes 12 days before delivery. On physical examination, clusters of vesicles were seen on the infant’s torso, periumbilical region, and pharyngeal, nasal, and conjunctival mucosa. No lesions were seen on the mother’s genitals or the placenta. PCR testing of samples obtained from the infant’s skin, conjunctivae, pharynx, and blood was positive for herpes simplex virus type 1 (HSV-1). The results of chest radiography, lumbar puncture, and liver biochemical tests were normal. A diagnosis of neonatal HSV-1 infection that was confined to the skin, eyes, and mucosa was made.
The mother reported no history of previous HSV-1 infection. However, a postpartum endocervical PCR assay was positive for HSV-1. In this case, a primary maternal infection late in pregnancy was thought to have led to ascending intrauterine infection and possibly preterm labour after prolonged rupture of membranes. Treatment with acyclovir was given. At 2 years of age, the child had no recurrences and was developmentally normal.
DOI: 10.1056/NEJMicm2035394
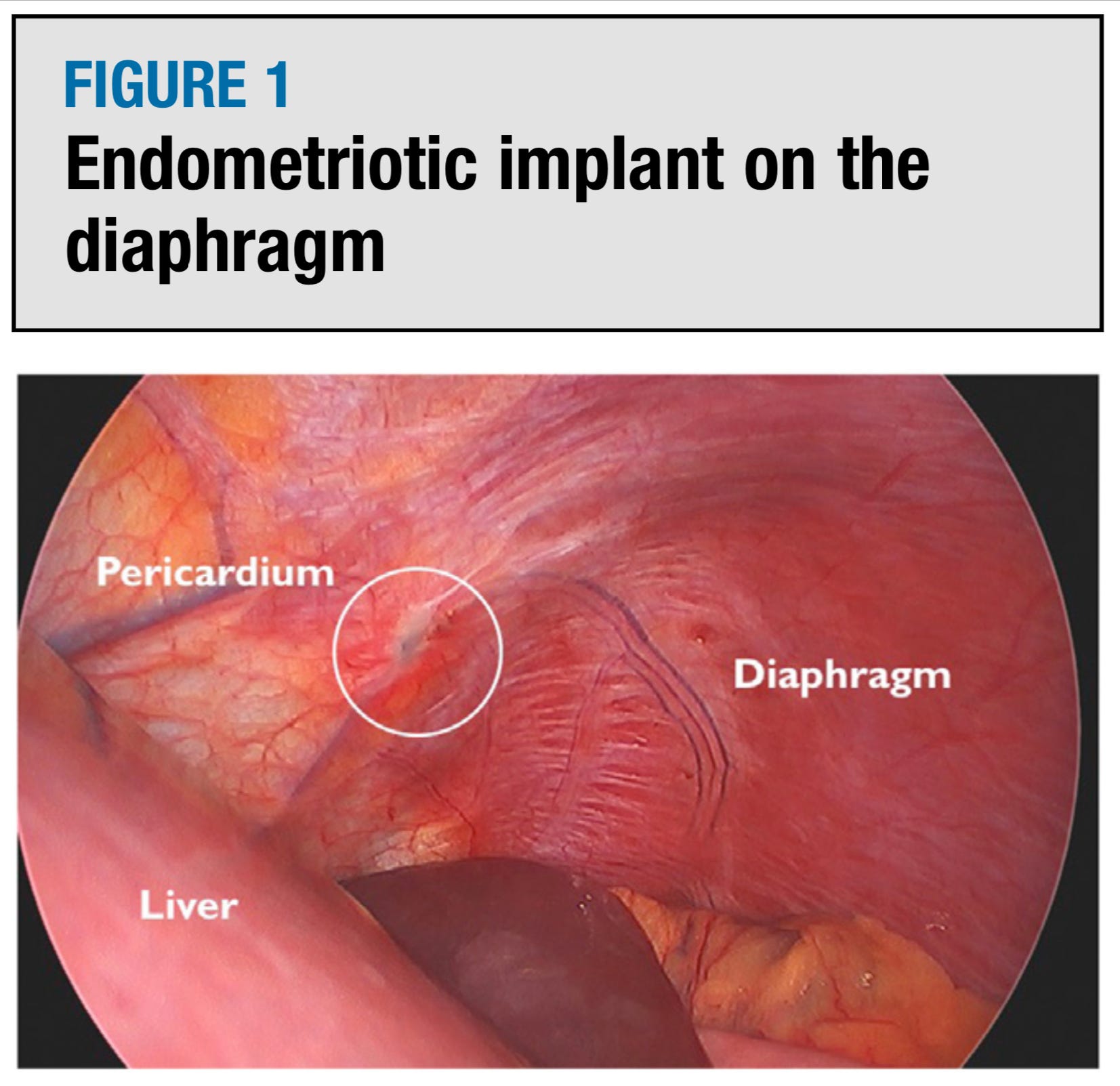
Surgeon’s Corner: Don’t forget to look up. Operating in the upper abdomen
Maternal fever in labour: aetiologies, consequences, and clinical management
This study investigated the association between intrapartum fever severity and neonatal/maternal morbidity. Results showed that composite neonatal morbidity increased with fever severity, while neonatal neurologic and maternal morbidity did not differ significantly between mild and severe fevers. The correlation between fever severity and neonatal morbidity was independent of duration from reaching maximum temperature to delivery, suggesting that clinical management should not be affected by this duration.
One-step total hysteroscopic removal of cervical ectopic pregnancy

A wider agreement is needed on basic intrapartum concepts
Healthcare professionals in labour wards face numerous challenges, such as long hours, emotional stress, and legal anxieties, which are exacerbated by a lack of consensus on fundamental intrapartum care concepts. Disagreements on issues like admission timing, labour progress, and pushing duration hinder the creation of a collective mental model crucial for effective teamwork and patient counselling. It is vital for international and national organisations to collaborate in establishing clear, globally-accepted guidelines to alleviate the burden on these professionals and improve the quality of care provided to patients.
Sexual functioning more than 15 years after premenopausal risk-reducing salpingo-oophorectomy
This study examined the long-term sexual functioning in women at increased familial risk of breast or ovarian cancer who underwent risk-reducing BSO either premenopausal (before age 46) or postmenopausal (after age 54). A total of 368 women aged 60-70 were included in the analysis. Results showed that the proportion of sexually active women was similar between both groups, with no difference in sexual pleasure scores. However, women who underwent premenopausal risk-reducing BSO reported significantly more discomfort during sexual intercourse and more severe complaints of vaginal dryness compared to their postmenopausal counterparts. Despite this, there was no reduction in sexual pleasure reported. No significant differences in pleasure or discomfort scores were observed between women who underwent the procedure before age 41 and those who had it between ages 41 and 45.
Management of term breech presentation

This review summarises the ongoing debate surrounding the optimal management of breech presentation at term, a condition affecting up to 5% of fetuses. Despite historical controversies dating back to Hippocrates, the issue remains unresolved in modern obstetrics. Vaginal breech birth (VBB) opinions vary widely among practitioners, with a general decline in enthusiasm for the procedure, although small groups in Australia continue to advocate for it. As some women will inevitably deliver breech babies vaginally, either by choice or necessity, it is crucial for obstetricians to have a thorough understanding of the practical aspects and evidence base. This article provides an updated overview of breech presentation at term, with a particular emphasis on VBB.