
Articles of interest
February 2024

Hey everyone,
Today’s email dives into a range of topics:
Two-layer vaginal cuff closure techniques in reducing postoperative complications following total laparoscopic hysterectomy, including a video of Dr Suketu Mansruia’s technique.
Timing of birth for small-for-gestational-age (SGA) fetuses in Queensland, aiming to balance the risks of stillbirth against neonatal morbidity.
Laparoscopic Reverse Submucosal Dissection method for treating rectosigmoid endometriosis, offering a less invasive alternative with promising patient outcomes.
The challenges of rising maternity care costs in Queensland, alongside deteriorating outcomes
Diagnosis of retained products of conception, highlighting the importance of accurate ultrasound criteria to prevent unnecessary interventions.
The impact of postpartum hypertension management on readmission rates is discussed, underscoring the critical need for effective hypertension control before discharge.
DRIGITAT: Doppler ultrasound in the management of late preterm SGA fetuses to improve clinical decision-making in suspected fetal growth restriction cases.
Finally, the concept of clinical debriefing is revisited, proposing a new framework to enhance its effectiveness in healthcare settings.
I hope these articles offer valuable insights and guidance for advancing your patient care in obstetrics and gynaecology.
Until next time,
Danny

Two-Layer Compared With One-Layer Vaginal Cuff Closure at the Time of Total Laparoscopic Hysterectomy
Vaginal cuff dehiscence is a significant concern following total laparoscopic hysterectomy, with a reported incidence of up to 5.8%. This study compared two-layer versus one-layer vaginal cuff closure techniques to determine their impact on postoperative complications.
The two-layer closure technique was associated with a significantly lower rate of vaginal cuff complications (0.9% vs 2.6%, P = 0.01) and overall postoperative complications (3.5% vs 5.7%, P = 0.01). These findings suggest that the two-layer closure may be a more effective approach to prevent postoperative complications following total laparoscopic hysterectomy.
SGA birth timing: Queensland analysis
Deciding the ideal timing for birth at term is a complex issue, balancing the escalating risk of stillbirth as gestation progresses against the potential for significant neonatal morbidity associated with early-term births. This concern is particularly acute for smaller infants. The objective of this study was to assess the risks of stillbirth, neonatal mortality, and severe neonatal morbidity by comparing expectant management with delivery from 37 weeks of gestation.
The risk of stillbirth escalated with gestational age, notably in infants with birthweight below the third centile, from 10.0 per 10,000 births at 37 weeks to 106.4 per 10,000 births at 40+6 weeks. Analysis indicated that the most suitable timing for birth varies based on birthweight centiles: 37+0 to 37+6 weeks for infants under the third centile and 38+0 to 38+6 weeks for those between the third and tenth centile. For all other centiles, birth from 39+0 weeks yielded the best outcomes - for the baby.

Laparoscopic Reverse Submucosal Dissection for infiltrating rectosigmoid endometriosis
Laparoscopic Reverse Submucosal Dissection (LRSD), first introduced in 2021, is a modified laparoscopic procedure for removing rectal endometriosis. This technique borrows from established hydrodissection methods in trans-anal gastrointestinal mucosal tumour treatments. In LRSD, a mixture of Gelofusine, vasopressin, and indigo carmine is injected into the submucosal layer of the rectum. This process helps to detach the muscularis, affected by endometriosis, from the mucosal layer. This study evaluates the outcomes in a group of women who underwent LRSD for symptomatic, deeply infiltrating rectosigmoid endometriosis, focusing on surgical, patient-reported, and safety results.
Danny Chou’s team at SWEC in Sydney and colleagues describe their technique and experience with 19 patients who underwent the procedure. Outcomes reviewed were surgical completion rate, VAS scores for endometriosis-related pain, QoL, constipation and incontinence scores. This technique builds on the partial thickness discoid excision approach, avoiding the risks of more invasive techniques such as full-thickness discoid excision (entry into the lumen) or segmental resection.

Maternity care in Queensland over time: more expensive, worse outcomes
During 2012–18, the demographic and clinical characteristics of women giving birth in Queensland changed, and the costs of maternity care increased at an unsustainable rate. This study quantified the value of maternity health care in Queensland based on outcomes and costs. The mean cost per birth increased from $20,471 to $30,000, and the proportion of births without adverse outcomes declined. Delivering high-quality maternity care requires strategies for containing costs while maintaining quality, and maternity care must focus on all dimensions of value.
Neither Queensland nor Australia is unique in its rise of intervention. With up to 1-in-3 women describing their birth experience as traumatic and objective perinatal PTSD affecting 4-9%, these data should make us reconsider how we - institutions and practitioners - provide care for women and babies in the future.
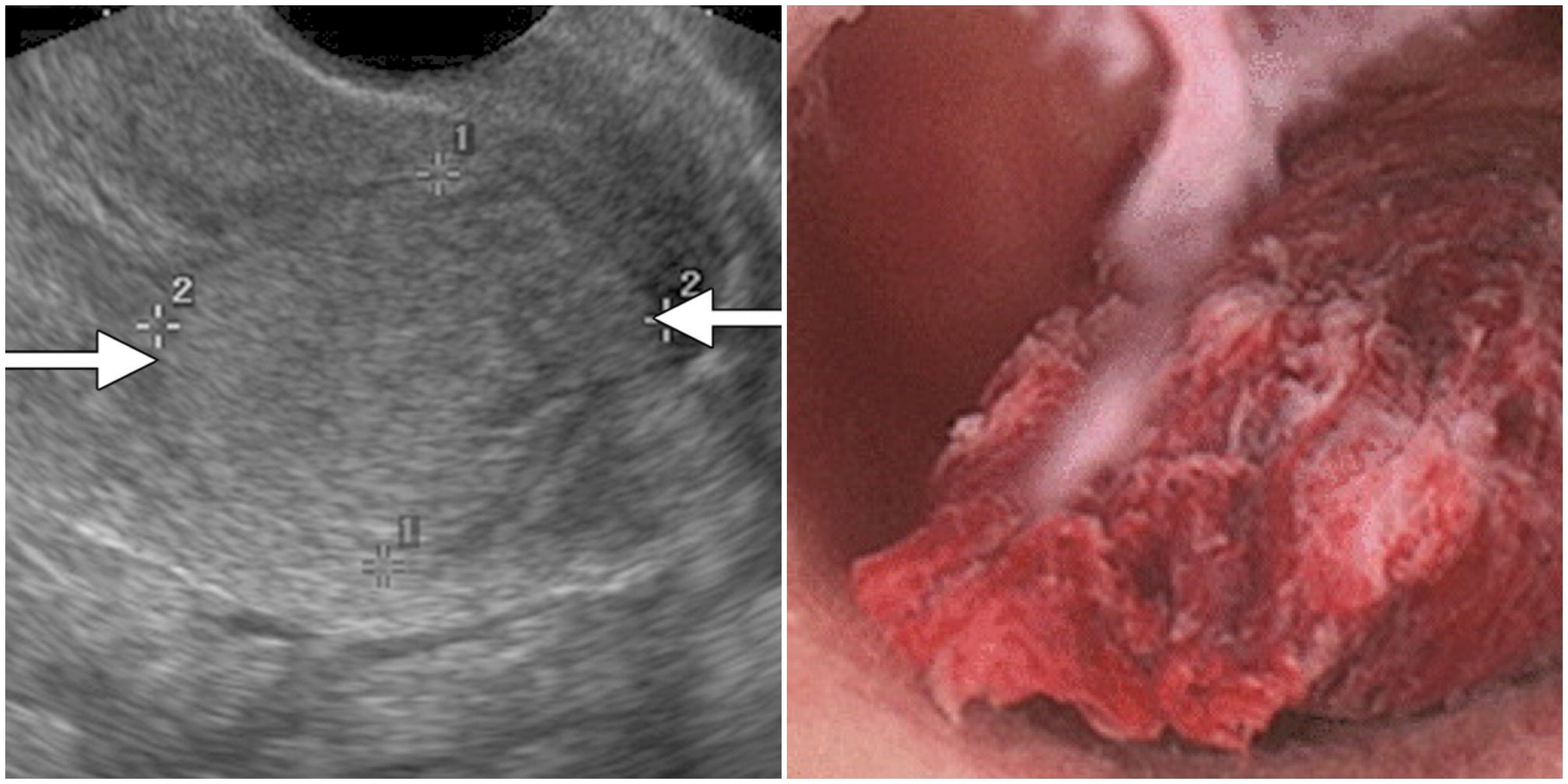
Diagnosis of Retained Products of Conception
Accurately diagnosing retained products of conception (RPOC) is essential to avoid complications like uterine perforation and endometritis from unnecessary surgery. Diagnostic approaches vary greatly due to uncertain diagnostic predictors, relying mostly on ultrasound and clinical symptoms. Prior reviews have failed to find a consensus on diagnostic ultrasound criteria. This systematic review assessed ultrasound modalities for RPOC, identifying echogenic mass as the most reliable indicator, more so than endometrial thickness or colour Doppler flow. It recommends combining echogenic mass with other ultrasound features for better diagnosis, advocating for standardised sonographic criteria to improve patient outcomes.
Sundararajan S, Roy S, Polanski LT. The accuracy of ultrasound scan in diagnosing retained products of conception: A systematic review and meta-analysis. American Journal of Obstetrics and Gynecology. 2023 Nov;
Postpartum management of hypertension and effect on readmission rates
Postpartum hypertension is a leading cause of maternal morbidity and mortality. This study investigates the association between hypertension 12 hours before discharge and the prescription of antihypertensive medications at discharge with hospital readmission rates.
Key findings:
Untreated hypertension within 12 hours before discharge was associated with a 32% higher risk of readmission in those who were not prescribed antihypertensive medications at discharge.
Women with hypertension in the 12 hours before discharge had a significantly increased risk of readmission, compared with those who were discharged normotensive, even when discharged with an antihypertensive prescription (adjusted odds ratio, 2.90; 95% confidence interval, 1.11–7.57).
These findings highlight the importance of treating hypertension to normalise blood pressure for at least 12 hours before discharge.
Lovgren T, Connealy B, Yao R, Dahlke JD. Postpartum management of hypertension and effect on readmission rates. American Journal of Obstetrics & Gynecology MFM. 2022 Jan;4(1):100517.
Doppler ultrasound of umbilical and middle cerebral artery in third trimester small-for-gestational-age fetuses to decide on timing of delivery for suspected fetal growth restriction: A cohort with nested RCT (DRIGITAT)
The detection and management of fetal growth restriction (FGR) remains a challenge in obstetrics, with suboptimal clinical outcomes for both the mother and fetus. This study aimed to improve the identification of FGR and guide clinical decision-making in late preterm small-for-gestational-age (SGA) fetuses.
Key findings:
New monitoring strategy: The study proposed using the umbilicocerebral ratio (UCR) as a marker for FGR in SGA fetuses from 32 to 36+6 weeks of gestation.
Higher risk: SGA fetuses with an abnormal UCR had a significantly higher risk of adverse perinatal outcomes, including perinatal death, birth asphyxia, and major neonatal morbidity.
Early delivery: Immediate delivery of SGA fetuses with an abnormal UCR at 34-36 weeks did not improve outcomes and may increase the risk of adverse events.
Expectant management: Expectant management until 37 weeks was associated with better short-term outcomes than immediate delivery.
Limitations: The study was halted early due to low recruitment rates, and larger studies are needed to confirm the findings.
Marijnen MC, Kamphof HD, Damhuis SE, Smies M, Leemhuis AG, Wolf H, et al. Doppler ultrasound of umbilical and middle cerebral artery in third trimester small‐for‐gestational age fetuses to decide on timing of delivery for suspected fetal growth restriction: A cohort with nested RCT (DRIGITAT). BJOG. 2024 Feb 5;1471-0528.17770
Routine versus prompted clinical debriefing: aligning aims, mechanisms and implementation
Clinical debriefing (CD) is gaining traction as a valuable learning and quality improvement activity in healthcare. However, its implementation faces barriers related to inconsistent terminology and a lack of understanding of the underlying mechanisms.
This research addresses these issues by proposing a new categorisation of CD into "routine" and "prompted" practices, highlighting their distinct aims and mechanisms. Routine CD is recommended for promoting learning from routine clinical events, while prompted CD aims to manage emotional responses or support psychological well-being following challenging events. The study emphasises the importance of aligning CD delivery with desired benefits and overcoming cultural barriers to implementation.1.
Phillips EC, Tallentire V. Routine versus prompted clinical debriefing: aligning aims, mechanisms and implementation. BMJ Qual Saf. 2024 Feb 2;bmjqs-2023-016836.